

BY BOB ALLER
In April 2017, at Vanderbilt University Medical Center (Nashville), a resident from the general surgery residency program was instructed to place a central venous catheter.
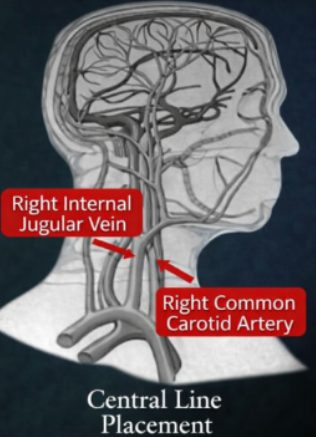
During the procedure in the morning (over 5 million central lines are placed each year), the resident missed the right interior jugular vein and mistakenly placed the central line in the patient’s right common carotid artery.
The medical error went unnoticed until mid-afternoon. At that time, the resident pulled out the central line and held pressure on the carotid for 30 minutes. The patient subsequently suffered a large right hemispheric stroke and passed the next day.
The following case report reviews key events leading to the patient’s death. This narrative is drawn from court records and the deposition testimony of Vanderbilt physicians who provided care for the patient.
Chaos In A General Surgery Residency Program

At 3:03 am on April 13, 2017, Chesta Shoemaker, a forty-four-year-old nurse, was admitted to the Vanderbilt ED in Nashville, Tennessee. At 3:49 am, an Emergency General Surgery consult by Dr. Sandra Kavalukas noted — ” … this looks like emphysematous pyelonephritis with extension into the peritoneal cavity and crossover into the portal system (a kidney infection had spread into the abdominal cavity and liver). Though stable, Ms. Shoemaker suffered from a serious infection. She was transported to the Surgical ICU.
General Surgery Resident Assigned

Second-year surgical resident Gretchen Edwards was assigned to Ms. Shoemaker. A critical care fellow, Dr. Richard Betzold, discussed the case with Dr. Edwards before she began the central venous catheter procedure at 7:45 am. The attending, Dr. Addison May, attested in a chart note that he was “personally present throughout the procedure.” Dr. Amanda Craig, an OBGYN intern, testified she was present to observe the placement of a central line.
Central Line Mistakenly Placed In Carotid Artery
Dr. Edwards attempted to place the catheter in the right internal jugular vein. However, she inadvertently placed the catheter (with a large-bore #9 catheter) in the right common carotid artery. Failing to recognize the error, Dr. Edwards noted in the chart that the procedure was “successful” with no immediate complications. At that time Dr. Edwards did not note whether she observed the color or pressure of the blood. The court records did not reflect any note made by the attending, Dr. May
Portable Chest X-Ray Taken To Confirm Central Line Placement Was Wrong

The radiologist, William Laxton, was deposed. Dr. Laxton admitted he had misinterpreted the film and his report had incorrectly reported the central line was properly placed.
Mrs. Shoemaker’s body was rotated slightly to the left, according to Dr. Laxton. She was rotated, but the rotation… didn’t give enough information to accurately tell where the actual catheter tip was… It was my best impression of the imaging that we had. …Due to subsequent imaging, I know that is not where the catheter tip ended up.
Patient Suffered Large Right Hemispheric Stroke
According to a court document, the cannulation of the carotid artery remained undetected for approximately 7 hours.
“Prolonged arterial cannulation can result in thrombus formation and stroke.”
At 6:05 pm, acting on a comment by a family member, the staff observed that Ms. Shoemaker had difficulty following commands and moving her extremities. A Code Stroke was called at 6:30 pm.
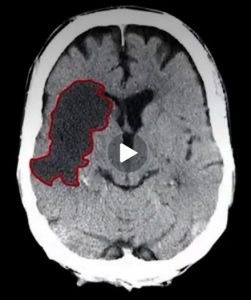
A CT angiogram showed a completely occluded right hemisphere of the brain. Chesta Shoemaker had suffered a large vessel stroke. A neuro exam revealed “brainstem dysfunction with possible progressive cerebral edema that could progress to brain death.” Ms. Shoemaker was transferred to the Neuro ICU. Though a thrombectomy was performed to remove the blood clot, it was too late. Recovery was not possible. Ms. Shoemaker’s family and friends came to be with her on her last day. Chesta Shoemaker’s life support was withdrawn on the evening of April 14, 2017. She passed at 10:26 pm. The Report of Death indicated the stroke resulted from “tearing of the right carotid artery.”
Death Certificate Included False Data

The death certificate completed by Vanderbilt Assistant Professor Dr. Eli Zimmerman certified Ms. Shoemaker died a natural death. Despite Dr. Zimmerman’s claim, Ms. Showmaker did not die a natural death according to a Tennessee standard. “If any external force or entity is related in any way to death, the manner of death cannot be considered natural.”
Lawsuit Filed Two Years Later

On February 11, 2019, a lawsuit was filed on behalf of Ms. Shoemaker’s adult son, Brett Keefer, in the Circuit Court of Davidson County, Tennessee. He had stayed with his mother during her two days at the hospital.
The deposition testimony of Vanderbilt doctors described with clarity the sequence of events leading to Ms. Shoemaker’s death.
Deposition Of General Surgery Resident, Dr. Edwards

Q: You agree that you punctured Chesta Shoemaker’s carotid when you attempted to place a central line in her jugular, on April 13th, 2017. Correct? Dr. Edwards: The catheter cannulated the carotid artery, yes.
Normally, the inadvertent cannulation of a carotid artery is promptly detected and corrected. However, in this case, Dr. Edwards failed to adhere to the Vanderbilt written policy requiring verification of central line placement with ultrasound or with pressure tubing of the placement of the guidewire. In her deposition, Dr. Edwards frankly admitted: “I did not trace the wire with ultrasound or use pressure tubing.”
Q: Were you aware of any written policies for placement of central venous access devices that were in existence at Vanderbilt University Medical Center on April 13, 2017?
Dr. Edwards: No.
Q: You were not following any written policy or procedure regarding placement of central venous access devices, on April 13, 2017, when you attempted to place a central line for Chesta Shoemaker. Correct?
Dr. Edwards: Correct.
Dr. Edwards testified she had previously placed 50 – 100 central venous catheters, while unsupervised.
Vanderbilt Policy For Central Venous Catheter
Court records indicated that Vanderbilt produced a copy of training materials and the hospital policy for the placement of a central venous catheter. The policy required verification of the placement of the central line with ultrasound or pressure tubing. Vanderbilt reported that Dr. Edwards received a copy of the policy prior to the treatment of Chesta Shoemaker.
The central line policy also indicated a nurse was required for a central venous catheter procedure. Yet, court records did not identify any nursing notes that substantiated a nurse was actually present during the surgery.
Dr. Edwards Testified She Was Unfamiliar With Ultrasound For Confirmation Of Central Line Placement
Q: You failed to use the ultrasound to confirm the placement of the catheter in Chesta Shoemaker’s jugular, on April 13th, 2017. Correct? Dr. Edwards: That is not a step I have seen performed in Vanderbilt Hospital.
Yet, Dr. Edward’s attending, Dr. Addison May, testified he supervised Dr. Edwards in the verification of central line placement using ultrasound.
Q: In your supervision of Gretchen Edwards in placing central lines, you would have trained and instructed her to verify placement of the finder needle with ultrasound guidance, correct?
Dr. May: Correct
Q: You would have instructed and trained her to verify placement of the guidewire with ultrasound guidance, correct?
Dr. May: Correct.
The critical care fellow, Dr. Betzold, was also deposed.

Q: … if you’re going to use ultrasound, do you instruct residents to use ultrasound not just with the finder needle but also to confirm placement of the guidewire?
Dr. Betzold: Yes.
Q: Did you teach or instruct at any time Gretchen Edwards regarding placement of central venous catheters?
Dr. Betzold: Yes.
Q: If you had assisted or observed Gretchen Edwards’ attempted placement of the central venous catheter on April 13, 2017, you would have ensured or insisted upon that additional confirmatory step. Correct?
Dr. Betzold: Correct.
Discovery Of Central Line Lodged In Carotid
Court records show that the puncture of the carotid artery was recognized at 3 pm. Both Dr. Betzhold and Dr. Edwards became aware of the medical error during a procedure to monitor Ms. Shoemaker’s cardiac function.
Drs. Betzold and Edwards placed a Swan-Ganz catheter through the same right-side central line placed by Dr. Edwards. When an arterial pressure waveform appeared on the monitor, they recognized that the central venous catheter was placed in the carotid artery.
Dr. Edwards Told To Consult Vascular Surgery
After discovering the misplaced central line, Dr. Betzhold personally placed a second central line on the left side of Ms. Shoemaker, verifying final placement with ultrasound. Dr. Betzold testified he called the attending, Dr. May, to report what happened. Dr. Betzold said he told Dr. Edwards to consult with Vascular Surgery (assigned for such an event). Dr. Betzold also said the call schedule would indicate the on-call attending physician (Dr. Curci).
Vanderbilt used a standard paging system or “call schedule” to reach Vascular Surgery. A call through the paging system to Vascular Surgery would have resulted in immediate support by the vascular team, including the attending, Dr. Curci.
Did Vanderbilt Require An Attending To Be Notified?
The court records and depositions do not specify if or when a Vanderbilt general surgery resident is required to notify an attending about critical medical issues. However, some general surgery programs specify precisely when a resident must contact an attending. For example, Stanford requires that a general surgery resident must contact the attending if any error or unexpected serious adverse event is encountered at any time.
Dr. Edwards Did Not Consult The Attending
Dr. Edwards, a second-year resident in this general surgery residency program at the time of the incident, was asked if she spoke to the attending.
Dr. Edwards: “Dr. Curci was the vascular surgeon attending…I did not discuss it with any attending physician… I discussed it with Dr. Julie Boll.”
Dr. Edwards failed to follow Dr. Betzold’s instructions to call Vascular Surgery (with access to the attending). Instead, she called Dr. Boll, (a vascular fellow), whose cell phone number was already in Dr. Edwards’s phone since Dr. Boll was a personal friend.

Q: Who told you to remove the catheter from Chesta Shoemaker’s carotid artery on April 13, 2017? Dr. Edwards: Dr. Boll. Q: Did she tell you to hold pressure on the carotid artery? Dr. Edwards: Correct. Q: Did she tell you how long to hold pressure on the carotid artery? Dr. Edwards: I don’t recall. Q: Have you ever even heard that it would be an appropriate thing to do to hold pressure on a patient’s carotid artery? Dr. Edwards. Yes. (In her testimony, Dr. Edwards said she held pressure on the carotid for 30 minutes.) Q: At the time you removed the catheter from Chesta Shoemaker’s carotid artery, you’d never been involved in a case where a patient’s carotid had been punctured before. Correct? Dr. Edwards: Correct.
Dr. Boll Denied Dr. Edwards Claim That She (Dr. Boll) Told Dr. Edwards What To Do
When questioned, Dr. Boll testified she never gave any instructions to Dr. Edwards. She was asked if she would have recommended pulling out the line in the patient’s room. “Absolutely not,” she replied. In addition, Dr. Boll testified she was not on call for vascular surgery when Dr. Edwards called her.
Dr. Boll: Vanderbilt General Surgery Residency Program Culture Permitted Residents To Circumvent Hospital Policy
Dr. Boll indicated that the “culture at Vanderbilt” established a “chain of command” for residents to call another house staff of their choice while bypassing the vascular surgery call schedule.
Dr. Boll: …This was a very normal circumstance. During my two years there, I had a least four central lines placed in the carotid artery.
Q: What do you remember Gretchen Edwards telling you about Ms. Shoemaker during that call? Dr. Boll: ...A line had been placed in the carotid artery in a patient that was in the ICU… And I said, because I was finishing up a procedure, that I was going to come upstairs and assess the patient. Q: What advice or recommendation, if any, did you give Gretchen Edwards during that phone call? Dr. Boll: None, I told her I would come upstairs… Traditionally, the management of a carotid involved in a central line placement is to take the patient to the OR for a neck exploration and to remove the line and assure patency of the carotid artery. I knew my plan was to go upstairs and personally assess the patient.
According to Dr. Boll, Dr. Edwards did not wait for her to arrive. Dr. Edwards removed the central line on her own.
In her deposition, Dr. Boll was asked about the proper way to remove a central line from an artery.
Dr. Boll: …The reason you take a line out of the carotid artery in the operating room is the artery – everyone’s arteries are layers. They’re layered like an onion. And so, when that line goes in it can push one of those layers down and cause a dissection. So the point of taking it to the OR is to make sure that when you repair that artery, you tack up any of those walls to keep the artery open.
Testimony Of Vanderbilt Neurologist Shilpi Mitall

Shilpi Mitall, MD
Dr. Mitall, a stroke neurologist who treated Ms. Shoemaker, was also questioned about removing a central line.
Q: What could happen if a patient had a catheter placed into their carotid artery that was then just pulled out as opposed to having vascular surgery repair the hole?
Dr. Mitall: I would not recommend doing that…when any foreign body is in any arterial distribution, that can be a source of thrombus. Now, when the catheter is taken out that can dislodge the superimposed thrombus in any patient… which can then subsequently may or may not go to the brain…
Ms. Shoemaker’s son, Brett Keefer, testified that Dr. Mittal had tested his mother’s brain function as he watched. After the test, she told him that his mother was clinically brain dead. He added: Dr. Mittal said she was sorry and she cried about what had happened.
Brett Keefer also testified that earlier in the day, right after the puncture of the carotid artery was discovered, Dr. Edwards came over to him in his mother’s ICU room and told him “they had nicked something.” She said she would apply pressure for 30 minutes to stop the bleeding. “Everything was fine,” Dr. Edwards said, according to Mr. Keefer.
“Severe Complications” From Immediate Withdrawal
The American Society of Anesthesiologists Task Force on Central Line Access issued Practice Guidelines for Central Venous Access, highlighting severe complications from immediate withdrawal.
Dr. Edwards Made A Significant Chart Entry In The Evening, After Learning About Her Puncture Of The Carotid Artery
The hospital central line policy indicated “monitor for pulsatile flow, raising the tubing slowly to evaluate flow under pressure.” According to a court document, after learning she had accidentally penetrated the carotid artery, Dr. Edwards created a chart note at 7:29 pm. “I noted return of venous-appearing non-pulsatile blood.”
Why Didn’t The Attending Correct The Surgical Error?

Dr. Addison May was the attending. After Dr. Edwards placed the catheter at about 7:45 AM, Dr. May signed a procedural note at 09:25 am: “I was personally present throughout the entire procedure.”
The claim of being “…personally present throughout the entire procedure” indicated direct supervision by Dr. May.
Witnesses were deposed to determine if Dr. May was actually present during the procedure. One witness was OBGYN intern Amanda Craig.

Q: Do you have any recollection of any interactions with Dr. May on April 13, 2018, with respect to Chesta shoemaker? Dr. Craig: Not that I can recall… He was not in the room when the line was placed.
The supervising Critical Care Fellow, Dr. Richard Betzold, was asked:
Q: Was Dr. Addison May present in Chesta Shoemaker’s room when Gretchen Edwards attempted placement of the central venous catheter? Dr. Betzold: Not that I recall.
Dr. Edwards was asked if Dr. May was present.
Q: Was Dr. Addison May the attending physician who was responsible for supervising you, present at the time you placed the central line for Chesta Shoemaker, on April 13, 2017?
Dr. Edwards: …Dr. May, in my recollection, was not present in the room during the procedure.
In addition, Vanderbilt University Medical Center confirmed in a response to the plaintiff’s complaint: “Dr. May was not present throughout the entire procedure.”
If Dr. May had been present, the puncture of the carotid artery would likely have been expeditiously repaired.
Dr. Edwards Didn’t Know Her Own Competency Rating
Dr. Edwards testified that she didn’t know whether she met competency requirements to conduct central line procedures without direct supervision. When attorneys requested the relevant Vanderbilt records, Vanderbilt refused to turn over those records.
Dr. Edwards Now Uses Ultrasound To Confirm
Dr. Edwards testified that since the death of Ms. Shoemaker she always uses ultrasound to confirm the placement of the guidewire in the jugular vein during central line placement. She said: “…as an additional step to confirm” proper placement.
In Dr. Bezthold’s deposition, he was asked how he felt now that Dr. Edwards confirms the placement of a central line with ultrasound each time.
Q: But that was a lesson that you hoped that she would learn and presumably are glad that she has done in the future, correct?
Dr. Betzold: Yes.
The depositions of the physicians point to systemic problems in this general surgery residency program.
Everybody Involved Was Involved In This Complication
Dr. Betzold was asked: Do you think you should take any responsibility for what ultimately occurred with Chesta Shoemaker?
Dr. Betzold: “I feel like everybody involved was involved in this complication.”
Dr. Betzhold said he did not think Vanderbilt had given Dr. Edwards adequate support: …we should be supporting the people that have complications instead of putting them on an island…
Does The Testimony Of Vanderbilt Physicians Indicate The Normalization Of Deviance?
The Normalization of Deviance in Healthcare Delivery happens all too frequently. Violations of best practices are normalized over time. Everything runs smoothly until, inevitably, a tragedy occurs.
- Dr. Edwards claimed she was unaware of an existing written hospital policy requiring verification of the placement of a central line. She said she had completed 50 -100 central line procedures while unsupervised. Both Dr. Betzold and Dr. May indicated they had instructed Dr. Edwards in the verification of the placement of a central line. Does Dr. Edwards’ testimony suggest that the general surgery residency program may have failed to ensure compliance with the hospital’s central line policy?
- Dr. May wrote: I was personally present throughout the procedure. Three witnesses, as well as Vanderbilt, claimed Dr. May was not present. Did Dr. May abandon the second-year resident?
- The Vanderbilt hospital central venous catheter policy called for a nurse to be present during the procedure and make specific chart notes. The court records did not reflect any required notes made by a nurse.
- Dr. Edwards disregarded the instruction to call Vascular Surgery. According to Dr. Boll, the Vanderbilt “culture” allowed residents to routinely circumvent the Vascular Surgery team assigned for an immediate consultation. Does Dr. Boll’s testimony suggest that the general surgery residency program may have failed to ensure that residents followed the hospital policy to call the vascular team assigned to provide assistance?
Commentary on the Vanderbilt general surgery residency program:
Pilots and airline passengers benefit from safety protocols. If a plane crashes, the pilot dies along with the passengers. Normalization of deviance is not acceptable to pilots. However, in medical care, the doctors who cause harm by normalizing deviance do not die.
When a medical mistake happens usually the medical professional feels terrible about it. A typical physician will be motivated to consider how to avoid the mistake in the future.
Rather than throwing a resident “under the bus” or accepting “accidents happen,” one of the questions that must be answered at Vanderbilt is whether there were departures from safety protocols. If there was a departure, the next question must be whether the deviation was accepted (normalization of deviance) by the institution. The testimony of Vanderbilt doctors describes behavior consistent with the normalization of deviance.
When safety protocols are repeatedly ignored, accidents aren’t really accidents.
Jerry Rogan, MD
Editorial Consultant: Suzan Shinazy
Hospital Watchdog thanks experts for their pre-publication review of this case report.
Ms. Shoemaker’s son, Brett Keefer, speaks about the lawsuit filed against Vanderbilt in a Nashville NBC affiliate television news story
Complaint filed on February 11, 2019, against Vanderbilt University Medical Center & Dr. Gretchen Edwards
Answer to the Plaintiff’s Complaint filed on May 13, 2019
Plaintiff’s Rule 25 Disclosures filed on February 15, 2020
5 Comments
Starr Barreto, the entire team at Hospital Watchdog sends our sincere condolences. Yes, Chesta's life mattered.
Chesta Shoemaker was my younger sister. I think of her almost daily and miss her greatly, and always will. She was an excellent nurse, who cared greatly for her patients. She followed procedures, took notes in great detail and loved the patients she cared for over the years. I wish the medical hospital she went to for help would have cared for her in the same manner. Skipping safety procedures should never be an option. She mattered.
Rest in peace my sweet sister. 💔
Those who report any safety issues are eventually taken out of the profession. Anything that costs the hospitals money. The "boards" and the hospitals are attacking medical professionals together . A witch hunt pursues, and that person will be labeled as disruptive, dangerous, and crazy .
Vanderbuilt Creates Its Own “Good to Go” Culture
William O. Cooper MD of Vanderbuilt University developed the Center of Patient and Professional Advocacy (CPPA) with programs designed to help hospitals identify and get rid of “disruptive” and “unprofessional” physicians who are whistleblowers, patient advocates, and follow medical (not corporate) guidelines…
Under the guise of promoting a “culture of safety and risk reduction” the CPPA rejects root cause analyses of physicians’ mistakes, errors, or accidents and instead relies on “unsolicited” but encouraged complaints from patients, nurses, and colleague physicians, and, in one published study, hidden operating room voice recordings to elicit evidence of surgeons’ behavior – all processed in secret to punish (and to fire) physicians deemed corporate risks…
All CPPA solicited and unsolicited materials, documents, and deliberations and findings are protected from discovery by peer review legislation dating back to 1986. Nothing can be verified by the targeted physician. All reporting to the National Practitioners Data Bank is virtually permanent, indelible, and career-ending…
Vanderbilt’s “CPPA currently partners with more than 180 hospitals and medical groups who have contracted with CPPA and executed Business Associates Agreements to utilize our Patient Advocacy Reporting System (PARS) and Co-Worker Reporting System (CORS) services. These partnerships have led to the creation of CPPA’s repository of more than 1.5 million patient complaint reports and co-worker observations associated with the practices of more than 75,000 physicians and advanced practice professionals.” Hospitals are encouraged to partner with Vanderbilt’s PCCA programs to cleanse their staffs of “disruptive” physicians.
From UnitedHealth Group: “Vanderbilt University Medical Center's (VUMC) program that encourages staff to report disruptive physician behavior has yielded results, Lena Weiner reports for HealthLeaders Media… Disruptive physician behavior can take many forms, from failing to return calls from the nursing station to lashing out at fellow clinicians, says William Cooper, director of the Vanderbilt Center for Patient and Professional Advocacy.” See: https://www.advisory.com/daily-briefing/2016/04/19/peer-reporting-can-help-end-disruptive-physician-behavior
The involved physicians will never admit fault as that would risk being labelled “disruptive” and ultimately targeted for dismissal. Furthermore, such “unprofessionalism” is not in the best interests of the hospital or its stakeholders…
I wrote a story for my local medical society about how "normalization of deviance" relates to medical care services- based on my personal experience as a patient and as a supporter for my elderly parents. SSVMS.org magazine, current issue page 30. https://issuu.com/ssvmedicine/docs/2002-ssvmed/1?e=5422997/76465391 page 30.